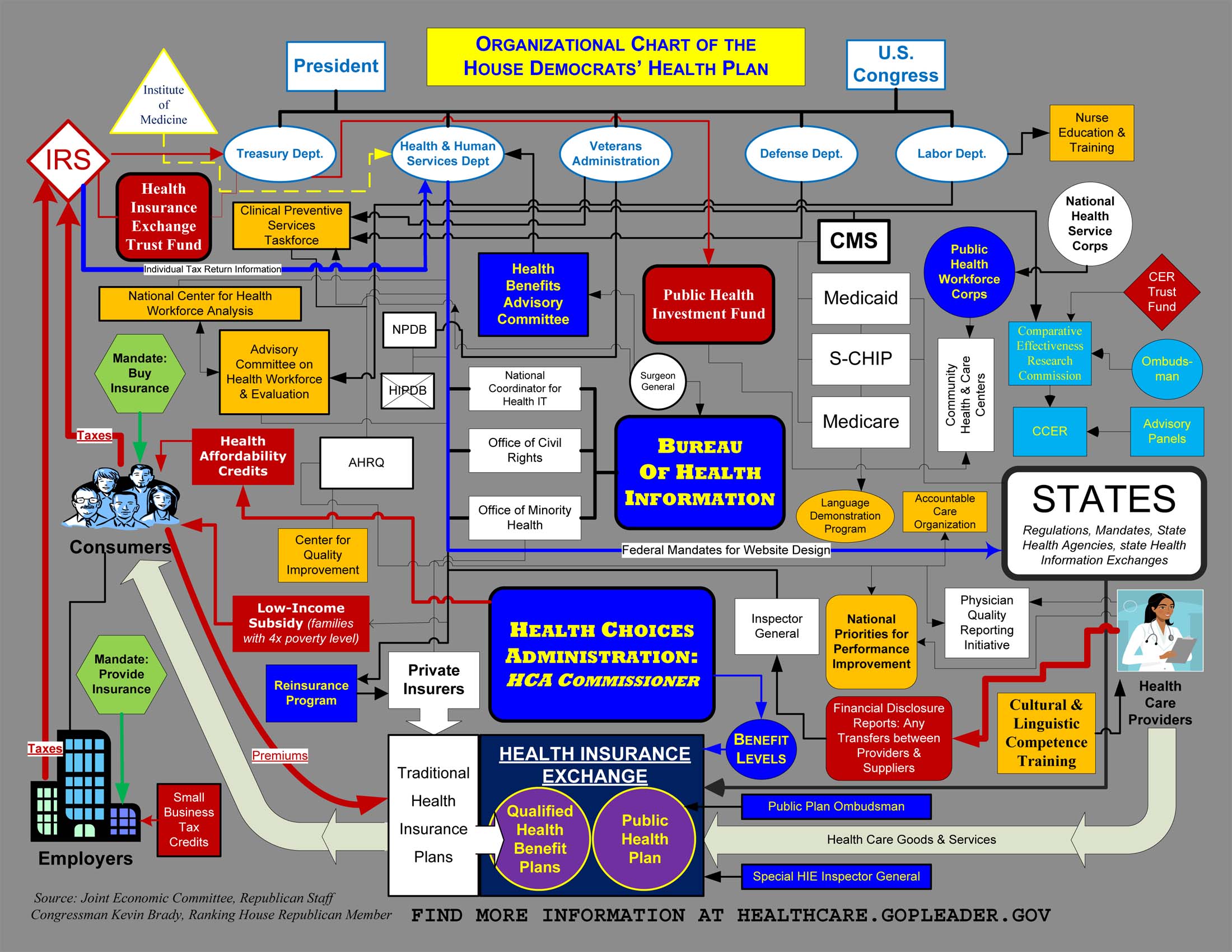
HINT: It’s enormous!
Speculation in a crisis
On the subject of masks, gloves, breathing machines, and pharmaceuticals:
Clichés of Socialiism #71
“Speculation should be outlawed.”
In 1869 John Fiske, noted American philosopher, scholar and literary critic, wrote an essay on “The Famine of 1770 in Bengal” (The Unseen World and Other Essays. Boston: Houghton Mifflin, 1876), Pointing out that a major reason for the severity of the famine was the Prevailing law prohibiting all speculation in rice. The following is excerpted from that essay.
THIS DISASTROUS piece of legislation was due to the universal prevalence of a prejudice from which so-called enlightened communities are not yet wholly free. It is even now customary to heap abuse upon those persons who in a season of scarcity, when prices are rapidly rising, buy up the “necessaries of life,” thereby still increasing for a time the cost of living. Such persons are commonly assailed with specious generalities to the effect that they are enemies of society. People whose only ideas are “moral ideas” regard them as heartless sharpers who fatten upon the misery of their fellow creatures. And it is sometimes hinted that such “practices” ought to be stopped by legislation.
Now, so far is this prejudice, which is a very old one, from being justified by facts, that, instead of being an evil, speculation in breadstuffs and other necessaries is one of the chief agencies by which in modern times and civilized countries a real famine is rendered almost impossible. This natural monopoly operates in two ways. In the first place, by raising prices, it checks consumption, putting every one on shorter allowance until the season of scarcity is over, and thus prevents the scarcity from growing into famine. In the second place, by raising prices, it stimulates importation from those localities where abundance reigns and prices are low. It thus in the long run does much to equalize the pressure of a time of dearth and diminish those extreme oscillations of prices which interfere with the even, healthy course of trade. A government which, in a season of high prices, does anything to check such speculation, acts about as sagely as the skipper of a wrecked vessel who should refuse to put his crew upon half rations.
The Capture of Antwerp
The turning point of the great Dutch Revolution, so far as it concerned the provinces which now constitute Belgium, was the famous siege and capture of Antwerp by Alexander Farnese, Duke of Parma. The siege was a long one, and the resistance obstinate, and the city would probably not have been captured if famine had not come to the assistance of the besiegers. It is interesting, therefore, to inquire what steps the civic authorities had taken to prevent such a calamity. They knew that the struggle before them was likely to be the life-and-death struggle of the Southern Netherlands; they knew that there was risk of their being surrounded so that relief from without would be impossible; they knew that their assailant was one of the most astute and unconquerable of men, by far the greatest general of the sixteenth century.
Therefore they proceeded to do just what our Republican Congress, under such circumstances, would probably have done, and just what the New York Tribune, if it had existed in those days, would have advised them to do. Finding that sundry speculators were accumulating and hoarding up provisions in anticipation of a season of high prices, they hastily decided, first of all to put a stop to such “selfish iniquity.” In their eyes the great thing to be done was to make things cheap. They therefore affxed a very low maximum price to everything which could be eaten, and prescribed severe penalties for all who should attempt to take more than the sum by law decreed. If a baker refused to sell his bread for a price which would have been adequate only in a time of great plenty, his shop was to be broken open, and his loaves distributed among the populace. The consequences of this idiotic policy were twofold.
In the first place, the enforced lowness of prices prevented any breadstuffs or other provisions from being brought into the city. It was a long time before Farnese succeeded in so blockading the Scheldt as to prevent ships laden with eatables from coming in below. Corn and preserved meats might have been hurried by thousands of tons into the beleagured city. Friendly Dutch vessels, freighted with abundance, were waiting at the mouth of the river. But all to no purpose. No merchant would expose his valuable ship, with its cargo, to the risk of being sunk by Farnese’s batteries, merely for the sake of finding a market no better than a hundred others which could be entered without incurring danger. No doubt if the merchants of Holland had followed out the maxim Vivre pour autrui, they would have braved ruin and destruction rather than behold their neighbours of Antwerp enslaved.
No doubt if they could have risen to a broad philosophic view of the future interests of the Netherlands, they would have seen that Antwerp must be saved, no matter if some of them were to lose money by it. But men do not yet sacrifice themselves for their fellows, nor do they as a rule look far beyond the present moment and its emergencies. And the business of government is to legislate for men as they are, not as it is supposed they ought to be. If provisions had brought a high price in Antwerp, they would have been carried thither. As it was, the city, by its own stupidity, blockaded itself far more effectually than Farnese could have done it.
In the second place, the enforced lowness of prices prevented any general retrenchment on the part of the citizens. Nobody felt it necessary to economize. Every one bought as much bread, and ate it as freely, as if the government by insuring its cheapness had insured its abundance. So the city lived in high spirits and in gleeful defiance of its besiegers, until all at once provisions gave out, and the government had to step in again to palliate the distress which it had wrought. It constituted itself quartermaster-general to the community, and doled out stinted rations alike to rich and poor, with that stern democratic impartiality peculiar to times of mortal peril.
But this served only, like most artificial palliatives, to lengthen out the misery. At the time of the surrender, not a loaf of bread could be obtained for love or money.
Rights vs. socialism
The American Constitution guarantees every citizen the right to access healthcare, education, jobs, homes, transportation, travel, public speech, their government, and many other rights.
No other country guarantees to its citizens all of the rights that Americans have.
American government is limited, but its citizens’ rights are not. For Americans, rights are unalienable, and within the bounds of law, practicable.
In other countries where rights are limited, government power is correspondingly greater. There’s an inverse relationship between government power and individual rights. They don’t coexist.
Socialists would have us trade away our unlimited rights for a smaller set of rights limited by government regulation, and a much larger basket of government powers. They would have us exchange freedom for government overseers.
Socialists use all sorts of emotional arguments to justify these trades, but in the end, they all lead to degrees of slavery.
Socialists who give up on the market, who give up the right to practice their rights as they personally see fit, make a very poor bargain for themselves, and for all who come after them.
Do you want the option to buy the healthcare you actually need? Or do you want a government bureaucrat to tell you what healthcare you are allowed?
Do you want the option to educate your kids in a curriculum you choose? Or do you want a government bureaucrat to determine what your child may learn at school?
Do you want to practice your own choices about what is best? Or do you want the government making those choices for you based on unproven dubious theories?
Do you want an economy run by consenting makers, sellers and buyers? Or do you want closed markets resistant to invention and creativity regulated by bureaucrats who have no personal skin in the game?
For reasonable people, these types of questions have obvious answers. Why do Leftists appear to lack the common sense necessary to see them?
The health industry
“It’s all about the money, boys!” Big Dan Teague
Health insurance, hospitals, big pharma, retail pharma, healthcare professionals, healthcare equipment and device manufacturing, are in it for the money. And rightly so. Money is the exchange medium that enables people to trade peacefully for what they want. Without money, people kill each other. See Venezuela.
Federal, state and local governments—political organizations—write laws to manage health care and health insurance. The laws they’ve written control prices, the services available, where those services will be provided, how much the patient pays, and most importantly, how much the government funds.
Political organizations follow the money. The biggest, most ossified and intransigent spender is government. Whoever turns that money spigot on gets rich.
That’s why congress isn’t repealing Obamacare. The reason has little to do with patient or voter revolts in 2018 that could favor Democrats, though Democrats certainly portray it as such—a case of making hay while the sun shines.
The reason comes from all of the vested money interests in the great mess of a health market enabled and protected by government. When it comes time to prune it back—i.e. now—no one will step forward to shut off their tap on the government money reservoir.
Politicians want to keep receiving money for their votes on profitable laws, begging the question of who profits.
Government health insurance/practitioner/substance/health transaction controllers and regulators all want to keep their statutory jobs.
Health finance at all levels of funds flow, a massive industry, want to keep their jobs.
And so it goes with the millions of consequential transactions all lubricated by virtually unlimited government money.
The patient entitlement is the tip of the iceberg. The far more pernicious entitlements in the fabric of the health industry—the ones that removal would lead to unemployment of the comfortably well paid—form the scaffold propping the whole thing up.
The mantra offered as a solution—“Single Payor”—would be like throwing gasoline onto a raging fire with the expectation it will perform like water.
The real solution is to reintroduce the highly protected and funded rare birds in all facets of the health industry to competition and market forces.
Because it’s all about the money, boys.
Drowning in good intentions
“1. The NHS provides a comprehensive service, available to all irrespective of gender, race, disability, age, sexual orientation, religion or belief. It has a duty to each and every individual that it serves and must respect their human rights. At the same time, it has a wider social duty to promote equality through the services it provides and to pay particular attention to groups or sections of society where improvements in health and life expectancy are not keeping pace with the rest of the population.”
The National Health Service Constitution
“The Constitution also contains pledges that the NHS is committed to achieve. Pledges go above and beyond legal rights. This means that pledges are not legally binding but represent a commitment by the NHS …”
health insurance claim denials
![]()
Who would go into a business where 15% to 25% of gross revenue is lost out the back end? Medicare is worse but commercial is almost as bad. The beneficiary model of health insurance is broken. No regulation the government is selling at either the Federal or State level is fixing or will fix this situation. Only market reforms that re-connect health care buyers to health care sellers, that re-establish supply and demand based pricing directly between market participants, that remove government regulation and payment systems from the entire process, and that stop empowering third parties to distort the health care transaction, can fix this market.
regulations ‘R’ us
List of New Bureaucracies in Obama’s Patient Protection and Affordable Care Act – PPACA
(Note: This is just from the enabling legislation. Each of these laws will spawn federal regulatory agency responses with tens of thousands of pages of CFR rules and federal bureaucratic enforcement. In classic Orwellian double speak, nothing about this legislation will make health care more affordable.)
1. Retiree Reserve Trust Fund (Section 111(d), p. 61)
2. Grant program for wellness programs to small employers (Section 112, p. 62)
3. Grant program for State health access programs (Section 114, p. 72)
4. Program of administrative simplification (Section 115, p. 76)
5. Health Benefits Advisory Committee (Section 223, p. 111)
6. Health Choices Administration (Section 241, p. 131)
7. Qualified Health Benefits Plan Ombudsman (Section 244, p. 138)
8. Health Insurance Exchange (Section 201, p. 155)
9. Program for technical assistance to employees of small businesses buying Exchange coverage (Section 305(h), p. 191)
10. Mechanism for insurance risk pooling to be established by Health Choices Commissioner (Section 306(b), p. 194)
11. Health Insurance Exchange Trust Fund (Section 307, p. 195)
12. State-based Health Insurance Exchanges (Section 308, p. 197)
13. Grant program for health insurance cooperatives (Section 310, p. 206)
14. “Public Health Insurance Option” (Section 321, p. 211)
15. Ombudsman for “Public Health Insurance Option” (Section 321(d), p. 213)
16. Account for receipts and disbursements for “Public Health Insurance Option” (Section 322(b), p. 215)
17. Telehealth Advisory Committee (Section 1191 (b), p. 589)
18. Demonstration program providing reimbursement for “culturally and linguistically appropriate services” (Section 1222, p. 617)
19. Demonstration program for shared decision making using patient decision aids (Section 1236, p. 648)
20. Accountable Care Organization pilot program under Medicare (Section 1301, p. 653)
21. Independent patient-centered medical home pilot program under Medicare (Section 1302, p. 672)
22. Community-based medical home pilot program under Medicare (Section 1302(d), p. 681)
23. Independence at home demonstration program (Section 1312, p. 718)
24. Center for Comparative Effectiveness Research (Section 1401(a), p. 734)
25. Comparative Effectiveness Research Commission (Section 1401(a), p. 738)
26. Patient ombudsman for comparative effectiveness research (Section 1401(a), p. 753)
27. Quality assurance and performance improvement program for skilled nursing facilities (Section 1412(b)(1), p. 784)
28. Quality assurance and performance improvement program for nursing facilities (Section 1412 (b)(2), p. 786)
29. Special focus facility program for skilled nursing facilities (Section 1413(a)(3), p. 796)
30. Special focus facility program for nursing facilities (Section 1413(b)(3), p. 804)
31. National independent monitor pilot program for skilled nursing facilities and nursing facilities (Section 1422, p. 859)
32. Demonstration program for approved teaching health centers with respect to Medicare GME (Section 1502(d), p. 933)
33. Pilot program to develop anti-fraud compliance systems for Medicare providers (Section 1635, p. 978)
34. Special Inspector General for the Health Insurance Exchange (Section 1647, p. 1000)
35. Medical home pilot program under Medicaid (Section 1722, p. 1058)
36. Accountable Care Organization pilot program under Medicaid (Section 1730A, p. 1073)
37. Nursing facility supplemental payment program (Section 1745, p. 1106)
38. Demonstration program for Medicaid coverage to stabilize emergency medical conditions in institutions for mental diseases (Section 1787, p. 1149)
39. Comparative Effectiveness Research Trust Fund (Section 1802, p. 1162)
40. “Identifiable office or program” within CMS to “provide for improved coordination between Medicare and Medicaid in the case of dual eligibles” (Section 1905, p. 1191)
41. Center for Medicare and Medicaid Innovation (Section 1907, p. 1198)
42. Public Health Investment Fund (Section 2002, p. 1214)
43. Scholarships for service in health professional needs areas (Section 2211, p. 1224)
44. Program for training medical residents in community-based settings (Section 2214, p. 1236)
45. Grant program for training in dentistry programs (Section 2215, p. 1240)
46. Public Health Workforce Corps (Section 2231, p. 1253)
47. Public health workforce scholarship program (Section 2231, p. 1254)
48. Public health workforce loan forgiveness program (Section 2231, p. 1258)
49. Grant program for innovations in interdisciplinary care (Section 2252, p. 1272)
50. Advisory Committee on Health Workforce Evaluation and Assessment (Section 2261, p. 1275)
51. Prevention and Wellness Trust (Section 2301, p. 1286)
52. Clinical Prevention Stakeholders Board (Section 2301, p. 1295)
53. Community Prevention Stakeholders Board (Section 2301, p. 1301)
54. Grant program for community prevention and wellness research (Section 2301, p. 1305)
55. Grant program for research and demonstration projects related to wellness incentives (Section 2301, p. 1305)
56. Grant program for community prevention and wellness services (Section 2301, p. 1308)
57. Grant program for public health infrastructure (Section 2301, p. 1313)
58. Center for Quality Improvement (Section 2401, p. 1322)
59. Assistant Secretary for Health Information (Section 2402, p. 1330)
60. Grant program to support the operation of school-based health clinics (Section 2511, p. 1352)
61. Grant program for nurse-managed health centers (Section 2512, p. 1361)
62. Grants for labor-management programs for nursing training (Section 2521, p. 1372)
63. Grant program for interdisciplinary mental and behavioral health training (Section 2522, p. 1382)
64. “No Child Left Unimmunized Against Influenza” demonstration grant program (Section 2524, p. 1391)
65. Healthy Teen Initiative grant program regarding teen pregnancy (Section 2526, p. 1398)
66. Grant program for interdisciplinary training, education, and services for individuals with autism (Section 2527(a), p. 1402)
67. University centers for excellence in developmental disabilities education (Section 2527(b), p. 1410)
68. Grant program to implement medication therapy management services (Section 2528, p. 1412)
69. Grant program to promote positive health behaviors in underserved communities (Section 2530, p. 1422)
70. Grant program for State alternative medical liability laws (Section 2531, p. 1431)
71. Grant program to develop infant mortality programs (Section 2532, p. 1433)
72. Grant program to prepare secondary school students for careers in health professions (Section 2533, p. 1437)
73. Grant program for community-based collaborative care (Section 2534, p. 1440)
74. Grant program for community-based overweight and obesity prevention (Section 2535, p. 1457)
75. Grant program for reducing the student-to-school nurse ratio in primary and secondary schools (Section 2536, p. 1462)
76. Demonstration project of grants to medical-legal partnerships (Section 2537, p. 1464)
77. Center for Emergency Care under the Assistant Secretary for Preparedness and Response (Section 2552, p. 1478)
78. Council for Emergency Care (Section 2552, p 1479)
79. Grant program to support demonstration programs that design and implement regionalized emergency care systems (Section 2553, p. 1480)
80. Grant program to assist veterans who wish to become emergency medical technicians upon discharge (Section 2554, p. 1487)
81. Interagency Pain Research Coordinating Committee (Section 2562, p. 1494)
82. National Medical Device Registry (Section 2571, p. 1501)
83. CLASS Independence Fund (Section 2581, p. 1597)
84. CLASS Independence Fund Board of Trustees (Section 2581, p. 1598)
85. CLASS Independence Advisory Council (Section 2581, p. 1602)
86. Health and Human Services Coordinating Committee on Women’s Health (Section 2588, p. 1610)
87. National Women’s Health Information Center (Section 2588, p. 1611)
88. Centers for Disease Control Office of Women’s Health (Section 2588, p. 1614)
89. Agency for Healthcare Research and Quality Office of Women’s Health and Gender-Based Research (Section 2588, p. 1617)
90. Health Resources and Services Administration Office of Women’s Health (Section 2588, p. 1618)
91. Food and Drug Administration Office of Women’s Health (Section 2588, p. 1621)
92. Personal Care Attendant Workforce Advisory Panel (Section 2589(a)(2), p. 1624)
93. Grant program for national health workforce online training (Section 2591, p. 1629)
94. Grant program to disseminate best practices on implementing health workforce investment programs (Section 2591, p. 1632)
95. Demonstration program for chronic shortages of health professionals (Section 3101, p. 1717)
96. Demonstration program for substance abuse counselor educational curricula (Section 3101, p. 1719)
97. Program of Indian community education on mental illness (Section 3101, p. 1722)
98. Intergovernmental Task Force on Indian environmental and nuclear hazards (Section 3101, p. 1754)
99. Office of Indian Men’s Health (Section 3101, p. 1765)
100. Indian Health facilities appropriation advisory board (Section 3101, p. 1774)
101. Indian Health facilities needs assessment workgroup (Section 3101, p. 1775)
102. Indian Health Service tribal facilities joint venture demonstration projects (Section 3101, p. 1809)
103. Urban youth treatment center demonstration project (Section 3101, p. 1873)
104. Grants to Urban Indian Organizations for diabetes prevention (Section 3101, p. 1874)
105. Grants to Urban Indian Organizations for health IT adoption (Section 3101, p. 1877)
106. Mental health technician training program (Section 3101, p. 1898)
107. Indian youth telemental health demonstration project (Section 3101, p. 1909)
108. Program for treatment of child sexual abuse victims and perpetrators (Section 3101, p. 1925)
109. Program for treatment of domestic violence and sexual abuse (Section 3101, p. 1927)
110. Native American Health and Wellness Foundation (Section 3103, p. 1966)
111. Committee for the Establishment of the Native American Health and Wellness Foundation (Section 3103, p. 1968)
Medical tourism


healthcare pricing bias
As the author says, “It’s worse than that.” The “bias to always raise prices” on the part of Medicare price fixers, is shared by manufacturers, suppliers, providers, insurers, and legislators who all have interests in putting more money into the system. The beneficiaries’ interests, the ones who ought to be providing demand input to the health care market to control pricing and supply allocation with their health care consumption free choices, are effectively muted. (click panels below to enlarge)
holy men vitamins
first impressions
The day began today in China (for us) with……Fox News! and the O’Reilly Factor–which works well as a morning talk show!
Fox News. Communist China. Go figure. Maybe it has something to do with Obama and Napolitano both on Fox today? Nice to see the left venturing outside their comfort zones on CNN and MSNBC.
(Update: Over in Shenzhen this afternoon–crossing the border from Hong Kong to China, we said goodbye to Fox News. 13 years into the 100 year merger of Hong Kong and China, looks like China proper will have to wait a little longer for Fox News.)
We read some illuminating articles in the China Daily (state) newspaper in transit. In a story about closing down ubiquitous unlicensed health clinics in China, the China Daily noted, “More than half of the rural population of China does not have adequate medical insurance.” The rural population is around 800 million. And migrant workers are not reimbursed for health care because people only get insurance reimbursement for fees incurred in the region they are from, not fees incurred in the region where they live and work. So, the government is trying to shut down market health care alternatives while also using health insurance as a tool to control migration.
On the next page of the 3/16/10 China Daily (page 9), an editorial says, “In the United States, the epitome of Western culture, it is difficult for a person without health insurance or enough money to get medical treatment. Visitors to the US, especially from poorer countries may be refused access to healthcare.” Well, this is simply misinformation. EMTALA guarantees health care to the point of stabilization to anyone who walks into a hospital emergency room. Moreover, it’s an unfunded mandate. Hospitals don’t get reimbursed for care provided under EMTALA.
It would be more productive for China to focus on health care provision for its uninsured and insured people than to obfuscate their own problems with straw man allegations about the U.S. system, which, though imperfect, is pretty good.
1 more week

not the party of no
GOP Idea Man Charts Course For Solvency
By GEORGE F. WILL
Posted 02/05/2010 06:25 PM ET
In 2013, when President Mitch Daniels, former Indiana governor, is counting his blessings, at the top of his list will be the name of his vice president: Paul Ryan. The former congressman from Wisconsin will have come to office with ideas for steering the federal government to solvency.
Not that Daniels has ever been bereft of ideas. Under him, Indiana property taxes have been cut 30% and for the first time, Standard & Poor’s has raised the state’s credit rating to AAA.
But in January 2010, Ryan released an updated version of his “Roadmap for America’s Future,” a cure for the most completely predictable major problem that has ever afflicted America.
Some calamities — the 1929 stock market crash, Pearl Harbor, 9/11 — have come like summer lightning, as bolts from the blue. The looming crisis of America’s Ponzi entitlement structure is different. Driven by the demographics of an aging population, its causes, timing and scope are known.
Funding entitlements — especially medical care and pensions for the elderly — requires reinvigorating the economy. Ryan’s map connects three destinations: economic vitality, diminished public debt, and health and retirement security.
To make the economy — on which all else hinges — hum, Ryan proposes tax reform. Masochists would be permitted to continue paying income taxes under the current system. Others could use a radically simplified code, filing a form that fits on a postcard.
It would have just two rates: 10% on incomes up to $100,000 for joint filers and $50,000 for single filers; 25% on higher incomes. There would be no deductions, credits or exclusions, other than the health care tax credit (see below).
Today’s tax system was shaped by sadists who were trying to be nice: Every wrinkle in the code was put there to benefit this or that interest. Since the 1986 tax simplification, the code has been recomplicated more than 14,000 times — more than once a day.
At the 2004 Republican convention, thunderous applause greeted George W. Bush’s statement that the code is “a complicated mess” and a “drag on our economy” and his promise to “reform and simplify” it. But his next paragraphs proposed more complications to incentivize this and that behavior for the greater good.
Ryan would eliminate taxes on interest, capital gains, dividends and death. The corporate income tax, the world’s second highest, would be replaced by an 8.5% business consumption tax. Because this would be about half the average tax burden that other nations place on corporations, U.S. companies would instantly become more competitive — and more able and eager to hire.
Medicare and Social Security would be preserved for those currently receiving benefits, or becoming eligible in the next 10 years (those 55 and older today). Both programs would be made permanently solvent.
Universal access to affordable health care would be guaranteed by refundable tax credits ($2,300 for individuals, $5,700 for families) for purchasing portable coverage in any state. As persons under 55 became Medicare-eligible, they would receive payments averaging $11,000 a year, indexed to inflation and pegged to income, with low-income people receiving more support.
Ryan’s plan would fund medical savings accounts from which low-income people would pay minor out-of-pocket medical expenses. All Americans, regardless of income, would be allowed to establish MSAs — tax-preferred accounts for paying such expenses.
Ryan’s plan would allow workers under 55 the choice of investing more than one-third of their current Social Security taxes in personal retirement accounts similar to the Thrift Savings Plan long available to, and immensely popular with, federal employees. This investment would be inheritable property, guaranteeing that individuals will never lose the ability to dispose every dollar they put into these accounts.
Ryan would raise the retirement age. If, when Congress created Social Security in 1935, it had indexed the retirement age (then 65) to life expectancy, today the age would be in the mid-70s. The system was never intended to do what it is doing — subsidizing retirements that extend from one-third to one-half of retirees’ adult lives.
Compare Ryan’s lucid map to the Democrats’ impenetrable labyrinth of health care legislation. Republicans are frequently criticized as “the party of no.” But because most new ideas are injurious, rejection is an important function in politics. It is, however, insufficient.
Fortunately, Ryan, assisted by Republican representatives Devin Nunes of California and Jeb Hensarling of Texas, has become a think tank, refuting the idea that Republicans lack ideas.
http://www.investors.com/NewsAndAnalysis/ArticlePrint.aspx?id=520346
British health system fails
As Congress acts on their leftist mythology to impose nationalized health care on America, the Brits document the folly of their own mistake.
Daily Mail, Saturday, November 28, 2009: 3,000 needless deaths every year
Daily Mail Comment, Saturday, November 28, 2009: Paying the ultimate price for NHS targets
The Daily Telegraph, Saturday, November 28, 2009: Want to fix the NHS? Go private
Senate socializtas
As the Senate considers socialized medicine for the U.S. today, consider what the concentration of government funding for socialized medicine throughout Europe has done for the business of health care. See Medica 2009 in Dusseldorf. It’s simply enormous. Floor space for the 4-day event costs around $20,000 for a 10′ x 10′ square. That’s $2M for a 100′ x 100′ space. The opulence is palpable. Massive displays of every medical device, machine, and product stretch for acres and acres in multiple linked buildings. Thousands of beautiful women and sharp dressed men represent their products with panache, elan and requisite sex appeal. The Medica show began around the same time governments began pouring public money into health care in the 60’s and 70’s. If you want more of something, subsidize it, and the evidence seems beyond doubt that public health care dollars have had this effect. It is puzzling, however, that the business of health care seems to be doing so well while the actual provision of health care seems to be in a state of crisis and in need of further socialization, more subsidy, and more government control. Is there really a disconnect here? Or is the argument for socializing health care in America a myth propagated by a leftist congress intent on perpetrating an extreme device to transfer more wealth and power to government forces? If the U.S. House and Senate get their way, we’ll definitely get more health care business. Ironically, we’ll also get health care rationing, scarcity of providers, and enormously increased taxes. Imagine how our economies would look without governments confiscating enormous wealth and directing it into favored industries, and instead, people directed the spending of their own wealth toward goods and services they actually wanted? Would we buy these fantastically expensive trade shows? I seriously doubt it. 
government at the people
Dems Go Nuclear
Posted 10/16/2009 07:54 PM ET
Health Care: Democrats seem set to use the “nuclear option” to ram their government health takeover into law. Bipartisanship already looked dead; now it looks extinct.
The health care revolution the Democratic Congress has planned — with its inevitable medical rationing, thousands of dollars in increased insurance premiums, and coverage of illegal aliens — may get placed on the familiar fast track used to spend hundreds and hundreds of billions of taxpayer dollars this year.
Instead of the 60 votes needed in the Senate if proper parliamentary rules were followed, passing this reshaping of the medical system as a “budget reconciliation” measure would mean only a simple majority was needed.
House Ways and Means Committee Chairman Charles Rangel, D-N.Y., accused of cheating on his taxes, last week held a hearing to let the House version of the health reform bill be passed this way. As the Washington weekly Human Events reports, Democratic leaders “have apparently invoked the ‘nuclear option’ to shut out Republicans and ensure the bill is passed before the end of the year.”
So all those “town hells” during the summer, where senators and congressmen were given an earful about passing secretly written thousand-page bills without reading them, will be ignored. [Read more…]
Coffman’s health care town hall
9/3/09 at Elbert County Public Health building. About 150 in attendance.
“Public Option” example in Colorado
price feedback
No Reform Without Skin In The Game
By PAUL D. TORTLAND | Posted Thursday, August 27, 2009 4:20 PM PT
The scenario is all too familiar, and plays out daily in my office. After evaluating a patient I recommend a particular course of treatment. More often than not, the first question from the patient is not, “How effective is the treatment?’ or “How safe is it?” Rather, the refrain is “Will my insurance cover it?” If I tell them, yes, your insurance will cover the treatment, their eyes glaze over and they couldn’t care less what their care will cost. If, on the other hand, the procedure is not covered, the bargaining begins: “Do you give cash discounts?” “Can I set up a payment plan?” Or, “That’s too much right now.”
It’s easy to spend someone else’s money. It’s a different story when your wallet is on the table. [Read more…]
bureaucracy care
click to enlarge
Caution: Don’t get sick.
health care debate we SHOULD have
In America, government fixes all Prices (called “fee schedules”) for health care devices, drugs, services, and procedures that are provided with public money (Medicare, Medicaid, Social Security, the VA, etc.) The private insurance market also uses these government fixed prices, but usually at a discounted rate–still price fixing, just at a discount.
Health care price-fixing happens at the political nexus where interest groups and lobbyists meet legislators and regulators. These politics do not yield the sort of equilibrium you get with the market forces of supply and demand. No one involved in establishing these price points actually has to pay for what they’re pricing. Therefore the demand element of this health care pricing mechanism is a fiction. Prices that come out of this process will only randomly reflect what real supply and demand would, and will only randomly be rational.
Meanwhile, legislators and regulators do not operate in a vacuum. They get ALL of their demand side pricing information from a) providers and b) insurance companies. They get ALL of their supply side pricing information from a) providers, b) insurance companies and c) manufacturers.
No inputs to health care price-fixing come from the actual consumers of health care, and the consumers of health care are the ONLY element in the health care market who are CAPABLE of providing real demand information–because they are the ones who actually pay for it!
To summarize, providers want higher health care prices because they earn more money that way. Insurance companies want higher health care prices because they earn more money on more expensive products and services. Manufacturers want higher health care prices because they earn more money for their goods. And legislators and regulators are disinterested third parties who exist to be persuaded to control price points, where all the persuasion comes from parties who have an interest in higher price points.
This is the debate we should be having. Any proposed structural change to our health care market that does not address what fundamentally controls the price of health care in America will not materially improve matters.
Our current system of health care pricing is disconnected from consumers and can only result in a poor allocation of health care to meet real needs. This is what we have today. If we don’t change this, we will never optimize the provision of health care, with the cost of health care, and with a rational price for that health care.
Government price fixing causes shortages–an economic fact of life whether the object is gasoline or health care.